
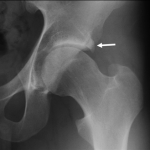
Femoro-acetabular impingement syndrome is a common cause of hip and groin pain and is probably the commonest cause of premature hip arthritis. FAI can affect both males and females and has a peak incidence between the age of 20-40. The cause of FAI is largely due to the shape of the hip bones. The hip joint is a ball and socket joint. If there is a shape mis-match between the ball and socket joint this can lead to premature damage to critical structures of the hip joint like the labrum and cartilage. Cam impingement occurs where there is loss of sphericity of the femoral head, leading to a bony bump. This cam bone shape may occur as a result of earlier hip problems such as Slipped Epiphysis, Perthes Disease, or Dysplasia. Patients with FAI Syndrome may have cam, pincer, or a combination of the two.




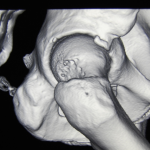
Pincer impingement is due to extra bone on the socket (acetabulum).
Pain can occur during activities as simple as sitting, and walking but is more common with activities which involve twisting, kicking, running, and extreme movements such as martial arts or Australian Football.
Physical examination is likely to demonstrate restricted range of movement of the hip joint and an impingement test is likely to reproduce typical hip/groin pain. A detailed review of your xrays, MRI and or CT scans will be undertaken to assess your hip joint for any cam or pincer bone shape, and associated damage to soft tissues.
Not all people with FAI Syndrome need surgery, but if you do, HAA can provide you with the most up to date treatments for FAI. In June 2018, The Lancet (one of the leading medical journals in the world), published a study confirming that hip arthroscopy surgery was better than physiotherapy/conservative treatment for FAI syndrome.
Hip Arthroscopy surgery can reshape your bones and repair damage to cartilage, labrum and other soft tissue structures within the hip joint. Most patients typically spend one night in hospital and will use crutches to help mobilise initially.
Postoperative rehabilitation is very helpful to improve the speed and quality of recovery. The hip will generally improve markedly over the first 2-6 weeks after surgery, but may continue to improve for up to 12 months after surgery.
Patients can expect their pain to improve significantly in the great majority of cases, particular if the surgery has been undertaken before any permanent damage occurs in the hip.
HAA has published a large number of studies on the surgical techniques and outcomes of their work (see HAA publications), so we can offer you reliable information on your likely outcomes based on our own experience and published results.